
Can Artificial Intelligence Out-smart a Cardiologist?
A landmark trial is showing how AI will help, rather than replace, specialist care

(IMPORTANT: this article is not medical advice, and has not been peer reviewed. You should consult your doctor if you have questions or feel unwell).
The high-stakes in heart care
In cardiology, our zip code is often our most significant risk factor. This is because for people with complex conditions like hypertrophic cardiomyopathy, a genetic predisposition to sudden cardiac death in young adults, proximity to elite medical expertise represents the literal line between life and death. And the stakes could not be any higher because timely diagnosis and the implantation of a cardiac defibrillator can virtually eliminate premature mortality. However, more than half of U.S. states lack a single hypertrophic cardiomyopathy subspecialist center. This is a structural issue that has left an estimated 60% of American hypertrophic cardiomyopathy patients undiagnosed. And this is not just a North American problem. As the global medical community braces for a projected deficit of 18 million providers by 2030, a landmark study recently published in Nature Medicine suggests that the solution to this specialist drought may not be found in medical school churning out more specialists, but in refined logic and computers. O’Sullivan and colleagues at Stanford University, in the USA have recently concluded a first-of-its-kind randomized controlled trial for articulate medical intelligence explorer, an AI system designed to upskill the generalist and democratize the rare knowledge of the elite subspecialist cardiologist.
The study
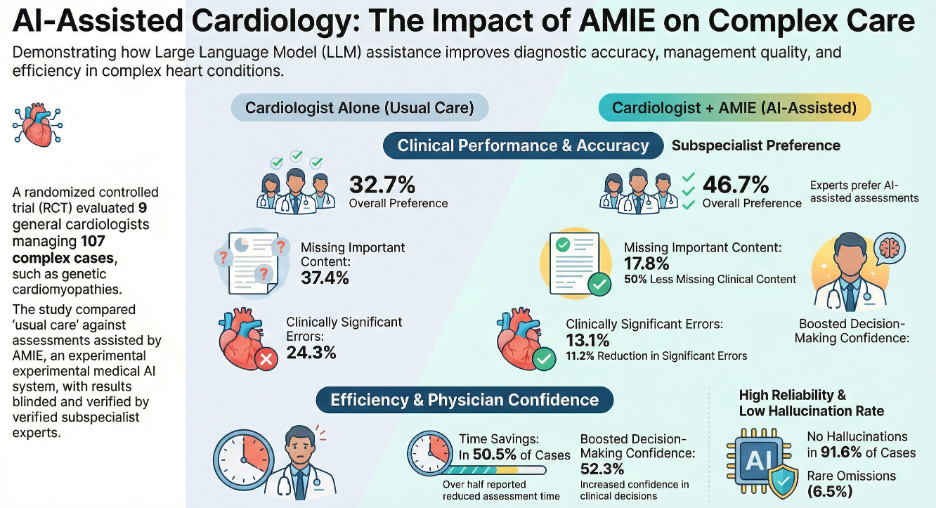
The trial centered on a whether an AI “co-pilot” could elevate a general cardiologist to the performance level of a world-class subspecialist. They used the Gemini 2.0 Flash architecture. Rather than relying on expensive fine-tuning, the researchers refined AMIE for this complex domain using just nine initial cases. Then, armed with this rapidly acquired expertise, nine general cardiologists managed 107 real-world cases involving a dense data stack of text reports from ECGs, echocardiograms, cardiac MRIs, and cardiopulmonary exercise testing. Statistically, when blinded subspecialists reviewed the results, they preferred the AI-assisted assessments in 46.7% of cases, compared to just 32.7% for cardiologists working alone. The subspecialists noted that the AI-assisted plans were significantly more comprehensive and better at incorporating modern diagnostics and advanced therapeutic interventions. As the World Health Organization warns of a collapsing global infrastructure. It predicts a deficit of 18 million providers by 2030. This disparity is further exacerbated for rarer and more complex conditions, particularly those for which timely treatment prevents morbidity and mortality. What is truly remarkable is the data from this randomized controlled trial, which show that an unassisted human baseline where cardiologists had a clinically significant error rate of 24.3%. With AMIE’s assistance, however, that rate was nearly halved to 13.1%. Perhaps even most importantly for the future of the medical workforce, the AI did not usurp the physicians, but enhanced them. This suggests that AI, rather than threatening professional ego, actually helps clinicians reclaim their cognitive margin by handling the exhausting work of data synthesis.
Efficiency against burnout
The trial results also offered a potential antidote to the pervasive burnout currently hollowing out the medical profession. AMIE proved to be an efficiency engine, saving doctors time in about 50% of cases. Most impressively, in nearly a quarter of all cases, the clinicians reported that the AI saved them more than 50% of their total assessment time. By automating the first-pass of data synthesis, AMIE allows the physician to transition from a data-entry clerk to a high-level curator. This shift in time allocation is crucial because it is the key to returning the human element to the bedside, even if the volume of patients spiked. The study also serves as a masterclass in why humans-in-the-loop will remain the gold standard. The reason is that AMIE recorded a 6.5% rate of clinically significant hallucinations, occasionally fabricating findings like “left ventricular hypertrabeculation” that were nowhere in the source data. A 6.5% rate of hallucinations may not seem much, but it is actually huge when the stakes are so high. The good news is that the study also finds that a collaborative-verification loop that happens when a general cardiologist challenged AMIE on the hallucinations, the AI system could frequently self-correct. This interaction is precisely what defines the co-pilot model as an awesome partnership between humans and AI. Here, the human provides the final mile of contextual reasoning and the AI provides the exhaustive data scan.
Conclusion
The initial fear of “AI vs. Doctor” is quickly dissipating and giving way to the era of “AI plus Doctor.” As AI begins to bridge the chasm between general practice and subspecialty care, the new question is whether the survival of a patient will depend less on geography and more on the quality of the partnership between a doctor and its digital co-pilot.